Fatigue from Slow COMT: The Fundamental Cause and How to Get More Energy
This is an article in a series I’m doing in response to the load of questions I received for my first AMA. Thanks to all who sent! I’ll be keeping these articles short and to the point. Excuse any typos here as I am typing/formatting fast so I can get through all your questions.
Near verbatim text of the question I received:
“I would like to find out more about the fatigue caused by the slow COMT gene and how to fix it thank you.”
A portion of my subscribers is here for Slow COMT specifically. I believe I’ve already addressed virtually all of the key points surrounding Slow COMT, at least more so than any other medical doctor at the time of this writing (not to brag…), and the issue of generic “fatigue” will ultimately extend from that broader COMT picture.
But let me go ahead and flesh out a few key points on fatigue specifically:
In short, if your fatigue really is from Slow COMT fundamentally, and not from some other tangential health issue, then:
this is ultimately a neuro-endocrine phenomenon arising originally from, of course, slow catechol breakdown.
As I hope you all know very thoroughly by now, Slow COMT causes a cascade of issues starting with poor breakdown of the catechols adrenaline, noradrenaline, dopamine, and catechol estrogens.
Side note: if you don’t already know the above, please read my other articles on slow COMT, some of which are linked here:
Slow COMT: The Definitive Clinical Guide for Testing and Optimization — Dr. Malek's MTHFRSolve
Don’t Take DIM if You Have Slow COMT (until you fix it) — Dr. Malek's MTHFRSolve
Should You Take Boswellia If You Have Slow COMT? — Dr. Malek's MTHFRSolve
What Supplements Should You Take if You Have a COMT Mutation? — Dr. Malek's MTHFRSolve
Supplements to Avoid with a Slow COMT — Dr. Malek's MTHFRSolve
Trapped Neurotransmitters: How Iron Deficiency Overloads a Slow COMT Brain — Dr. Malek's MTHFRSolve
Slow COMT in the Context of Sulfur Intolerance — Dr. Malek's MTHFRSolve
How the COMT Gene Affects Your Susceptibility to Pain — Dr. Malek's MTHFRSolve
How NAC Can Help People with COMT Mutations — Dr. Malek's MTHFRSolve
Ultimately that creates a high baseline tone of these biologically active catechol molecules. This can lead to fatigue through two PRIMARY routes:
FIRSTLY:
Slow COMT can cause fatigue by contributing to what is essentially an “adrenal fatigue” sort of picture
and yes, I do think adrenal fatigue is a real thing, however it may vex my fellow allopaths…
Elevated catecholamines lead downstream to elevated cortisol levels produced by the adrenal gland, make you feel wired and stressed in a whole-body sense, beyond the neurological elements.
Over much time, this can lead to a situation where your adrenal gland becomes resistant to further cortisol production (either by depletion or by complex changes in high-level signaling), eventually leading to low cortisol level even when your body needs them to be high, like in the early morning.
You can test for this phenomenon by doing whole-day 4-point cortisol testing, and, even better, by also testing your cortisol awakening response (and I do both in my clinic, fyi).
Ultimately, the Slow COMT Roadmap is designed to help fix this issue from a genetic root-cause perspective. You can find it inside Roadmaps to Health.
SECONDLY:
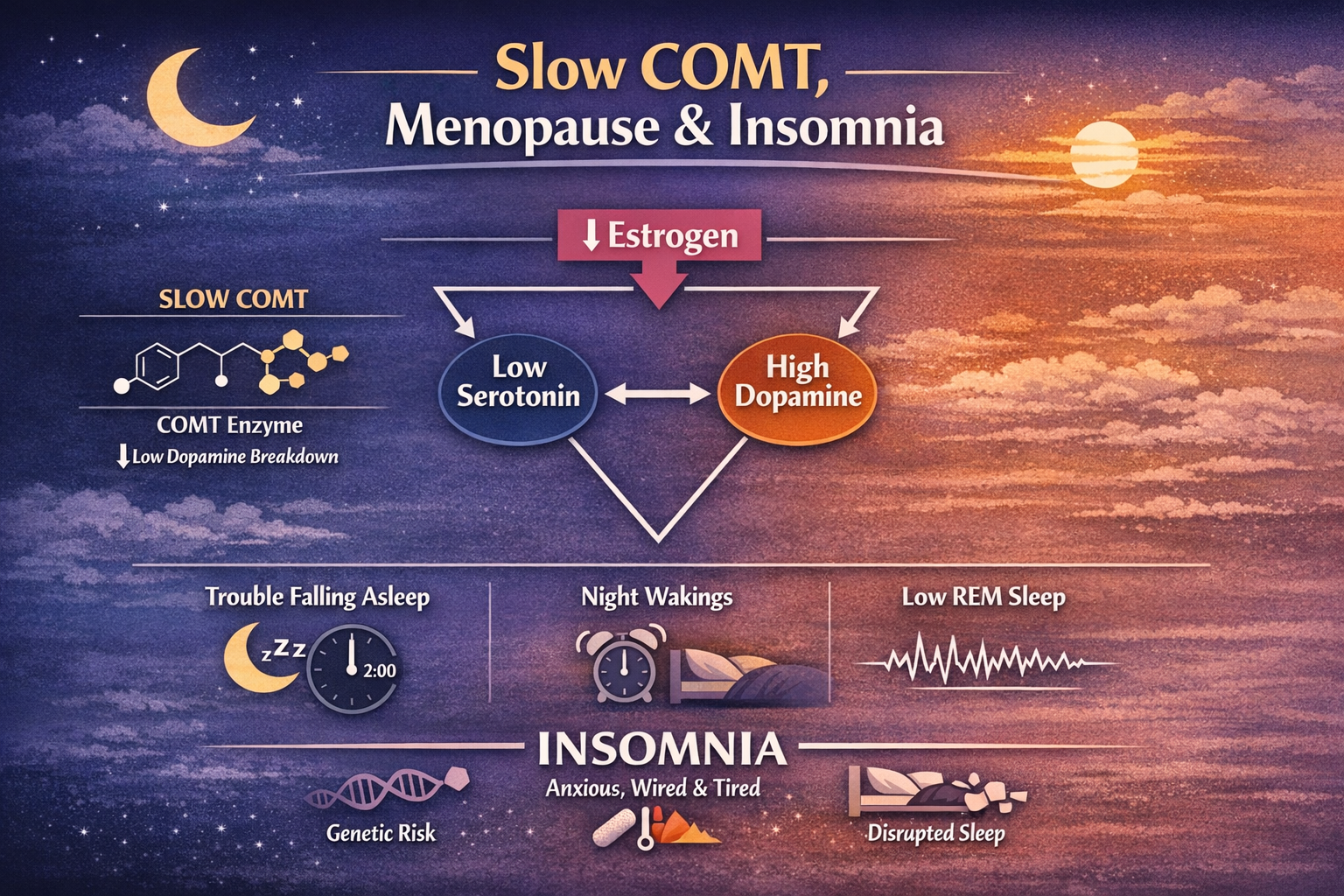
Slow COMT can cause fatigue via its effects on estrogen metabolism.
Long-story-short, it can cause an estrogen dominance situation, which very characteristically contributes to fatigue. I don’t have time and energy to discuss the full mechanism of this one, but I have built an entire Estrogen Detoxification Roadmap inside my Roadmaps to Health subscription that is designed specifically to fix this issue:
Estrogen Detoxification Roadmap
The subscription also includes a private Facebook group where you can ask questions and get direct answers. Thanks for your support!
EVERYTHING in this article is purely educational and informational in nature. None of this is medical advice. Make no health changes based on this article. I am not your doctor. Discuss any and all implementations with your own doctor.
READ MORE:










5th question I received:
“I would like to find out more about the fatigue caused by the slow COMT gene and how to fix it thank you.”