How Can Someone Be B6 Deficient and B6 Toxic at the Same Time?
This is an article in a series I’m doing in response to the load of questions I received for my first AMA. Thanks to all who sent! I’ll be keeping these articles short and to the point. Excuse any typos here as I am typing/formatting fast so I can get through all your questions.
Near verbatim text of the question I received:
“How can someone be both cellularly deficient in B6 while also being b6 toxic, and what are the methylation issues potentially preventing healthy utilization regardless of the form ingested?”
This question would require approximately 2 hours over video to properly address, so I’m not going to attempt that. Instead I’ll focus on one central aspect of the question.
Firstly (as I have to frequently caveat given the surprising sensitivity of this particular topic), I DO NOT at all endorse the standard “cellular deficiency” narrative of B6 that is touted by some ostensibly alternative practitioners and doctors, whereby they mean that a high plasma level of B6 always indicates poor cellular delivery, thus requiring high-dose P5P to remedy.
This is completely false.
The plasma B6 tested by most labs is P5P (i.e. PLP or pyridoxal-5-phosphate, the active form of B6). So when you go to Quest or Labcorp and get your B6 tested, what you’re testing is the active B6 floating around in the plasma component of your bloodstream.
So the supposed cellular deficiency issue is absolutely not remedied by giving yet MORE of that same form of B6.
Even beyond this elementary mistake, only a fraction of supposedly “B6 toxic” cases are characterized by poor delivery of B6 internally, so it is not correct to assume that all or even the majority of B6 toxic patients need to undergo some form of intracellular delivery rectification regimen.
Testing is almost ALWAYS the right next step.
I also want to address the element of methylation involved in this question. Specifically:
Is methylation involved in B6 toxicity (including MTHFR deficits/mutations etc.)?
The short and technical answer is no.
No major step involving the direct assimilation or metabolism of B6 involves a methylation reaction.
In other words, your MTHFR mutation is NOT responsible for your B6 toxicity, if you do in fact have B6 toxicity.
HOWEVER, some medical cases that are rashly considered to be bona fide B6 toxicity are not in fact B6 toxicity and do involve methylation. BUT every single such case is highly idiosyncratic and therefore cannot at all be blocked into one category of “B6 methylation issues.” I might write or speak more on this topic on the future if there’s interest.
That’s really all I can say generically on this issue.
Join my private Roadmaps Subscription + Facebook group to ask questions and get direct answers. Join here:
EVERYTHING in this article is purely educational and informational in nature. None of this is medical advice. Make no health changes based on this article. I am not your doctor. Discuss any and all implementations with your own doctor.
READ MORE:










5th question I received:
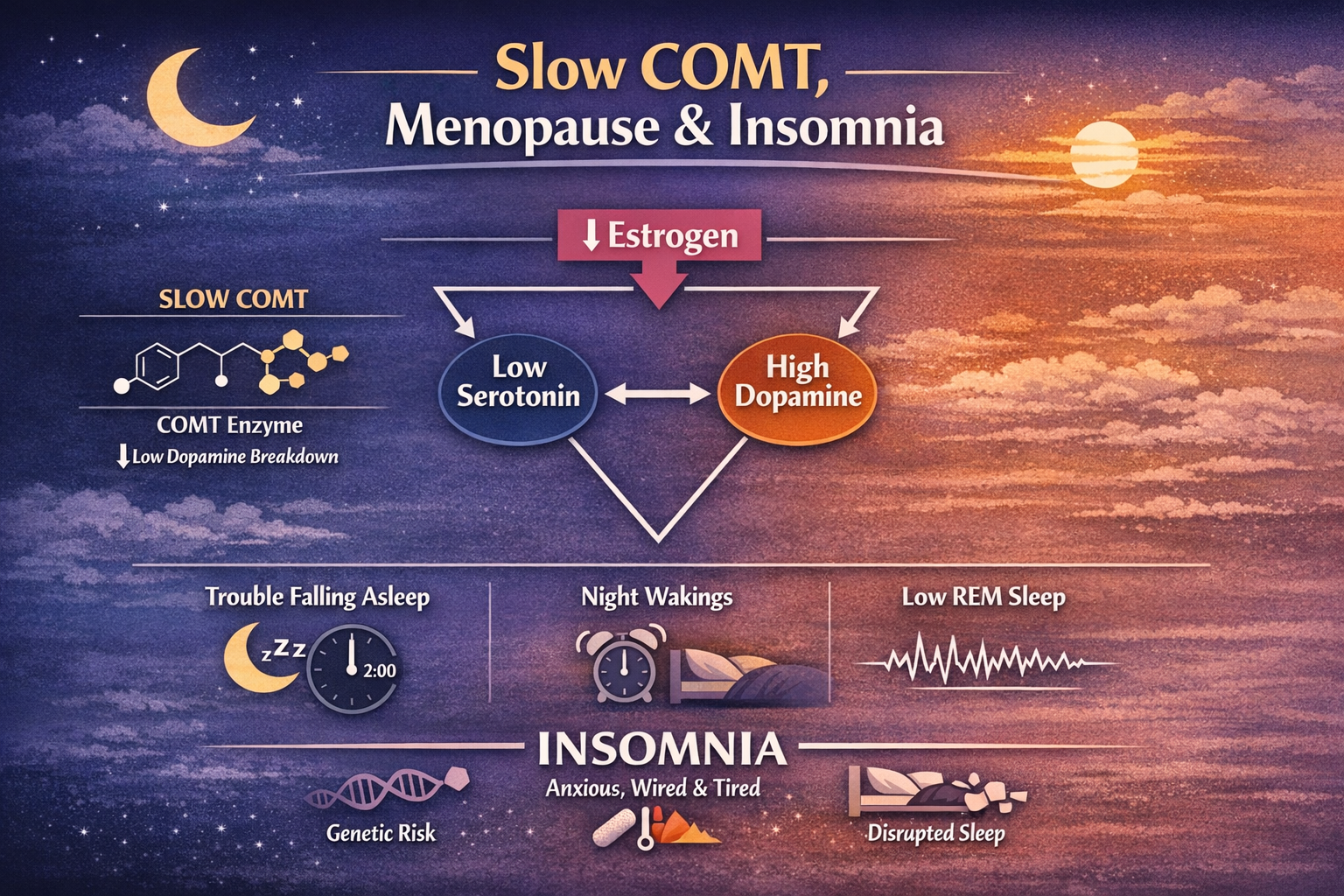
“I would like to find out more about the fatigue caused by the slow COMT gene and how to fix it thank you.”