Do You Ever Stop MTHFR Supplements? When Nutrients Can Be Temporary vs Lifelong
This is the first article in a series I’ll be doing in response to the load of questions I received for my first AMA. Thanks to all who sent! I’ll be keeping these articles short and to the point. Excuse any typos here as I am typing/formatting fast so I can get through all your questions.
Near verbatim text of the question I received:
“Once you support deficiencies and associated pathways with certain nutrients will you no longer need to take those supplements? Will the body be become independent of those supports over time or, because of certain genetic issues, will support always be needed?”
Note that, instead of talking about “pathways” in the general here, I’ll be focusing on MTHFR/methylation issues specifically to simplify the answer and provide a practical example for what I consider to be ultimately a high-level question regarding medical theory.
Do You Ever Stop MTHFR Supplements? Is this a temporary Fix or Lifelong Support?
The short answer is: It entirely depends on the nature of the issue that you’re correcting.
There are a few possible scenarios:
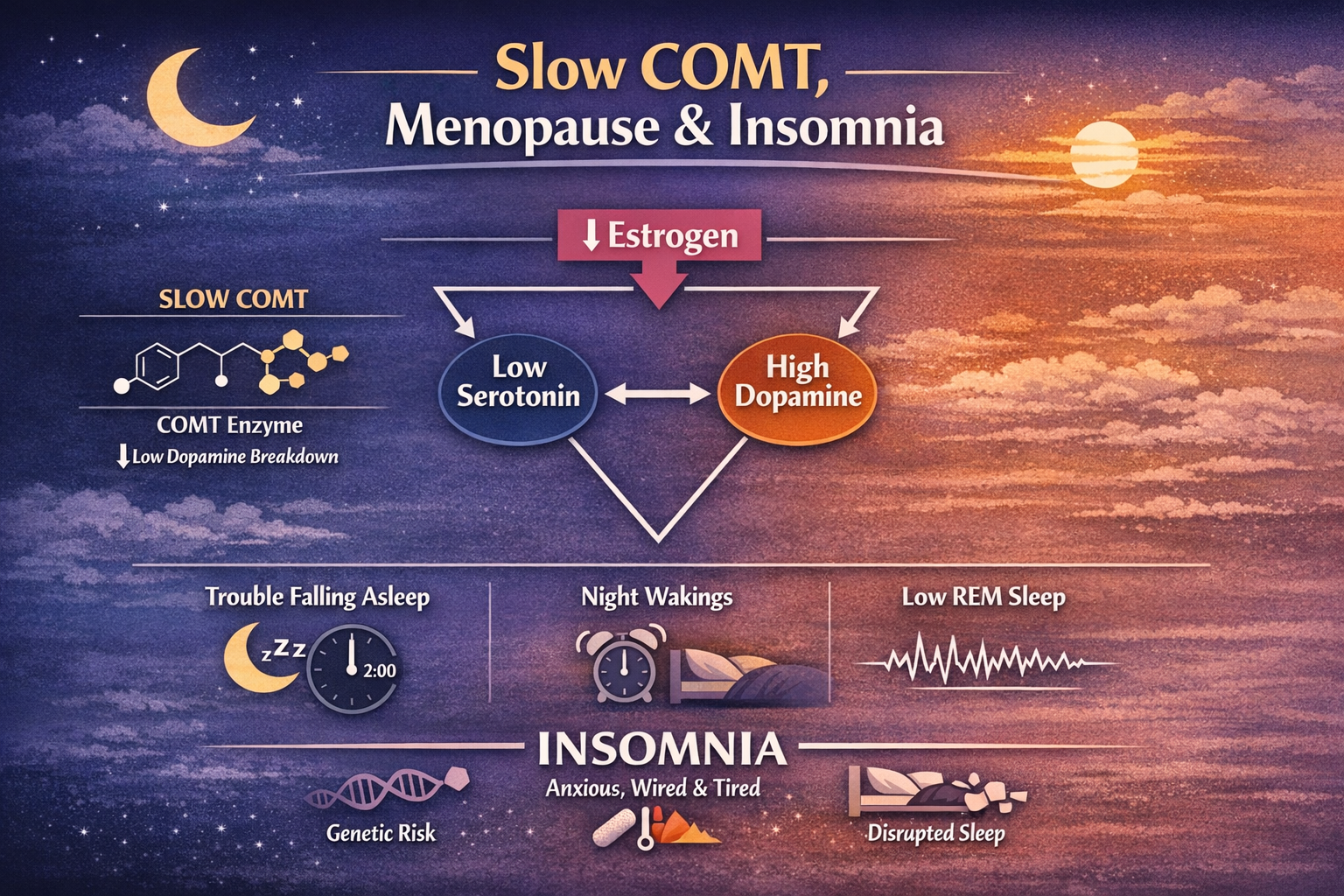
FIRST: If the issue is purely a genetic one (e.g. compound MTHFR variants with added MTRR/BHMT deficits etc. or Slow COMT), then it’s much more likely to require long term compensation; however, that lifelong compensation generally can eventually be narrowed down to just one to three supplements.
SECOND: If the issue is purely environmentally mediated, then you’re much less likely to require long term supplementation. Many methylation deficits, for example, or detoxification deficits (affecting liver metabolism, sulfation, etc. etc.) are environmentally mediated and do not require lifelong supplemental or nutritional compensation, you just supplement until you can be reasonably sure that you have sufficiently outdone the environmental deficit.
Those first two scenarios are, of course, incredibly uncommon, because most (really, virtually all) health issues are the THIRD OPTION: a combination of genetics and environment.
This applies 100% to methylation.
Whereas most of the online discussion surrounding methylation treats it as a purely genetic problem, that is entirely not the case…
Genetics mediates your underlying predisposition to methylation issues. It does not determine whether or not you will ultimately “get” “undermethylation” or any of the downstream functional or symptomatic issues characteristic of methylation deficits.
So even if you have MTHFR C677T homozygous (which is the most impactful form of the gene locus!), you’re not guaranteed to have issue with methylation. It’s just that you’re much much more likely to do so.
The issue, of course, is that the modern world makes methylation issues so much more consequential and so much more likely because we are indeed surrounded by factors that drain methylation on the daily.
Arsenic exposure is an excellent example of toxic exposure mediating undermethylation.
Poor nutrient density (which is potentially happening to virtually anyone eating food from a grocery store) is an example of paucity mediating methylation problems.
And even a tiny nudge from either of those two ubiquitous things above is enough to push MTHFR C677T homozygous into being functionally and symptomatically meaningful.
All that is to say: MOST people with health issues are in a situation that is a combination of genetic and environmental factors.
In those cases, whether or not you need to take supplements forever, and which ones exactly, is a much more complex situation than a theoretically “pure” genetics-only or environment-only situation.
MTHFR and Arsenic, as an example
As an easy example (and most are frankly much more complicated):
Let’s say we do indeed have someone with MTHFR C677T homozygous as well as arsenic exposure due to drinking their well water and poor nutrient density due to being human in the 21st century (lol)..
In this case, I’d likely begin such a person by very precisely targeting arsenic removal and mitigating the harmful effects of arsenic while also doing things that would increase the regeneration of SAMe at a rate greater than they would need indefinitely.
Doing that too long would actually become harmful eventually, serving the opposite effect.
We’d need to retest arsenic values, do some testing for deeper tissue exposure (HTMA can help although not 100% reliable), and, most importantly:
we have to TEST to determine the efficacy of our mitigation of the secondary effects of arsenic exposure.
Ultimately, however, once the acute arsenic load is removed and we verify that the above labs have in fact moved in response to what we’re doing, that person could probably suffice on 1-2 daily supplements and maybe a couple more taken intermittently, assuming only the problems mentioned above.
This is why the single most important thing to do here is to be extremely systematic about what you take and be extremely systematic about retesting and tracking.
Therefore, most importantly and in conclusion:
Your ability to be systematic and to determine that what you are trying to affect with your supplements actually is in fact changing in response to what you’re taking entirely determines how long you have to be on that stuff!
Join my private Roadmaps Subscription + Facebook group to ask questions and get direct answers. Join here:
EVERYTHING in this article is purely educational and informational in nature. None of this is medical advice. Make no health changes based on this article. I am not your doctor. Discuss any and all implementations with your own doctor.
READ MORE:







5th question I received:
“I would like to find out more about the fatigue caused by the slow COMT gene and how to fix it thank you.”