Don’t Take DIM if You Have Slow COMT (until you fix it)
One of the more common mistakes made by people with estrogen dominance is taking DIM by itself (and note that this can include postmenopausal women on HRT/Hormone Replacement Therapy).
DIM is a powerful estrogen metabolism modulator derived (as is less commonly known) from cruciferous vegetables like broccoli and cauliflower. That shouldn’t be too surprising for those aware of the quite broad and heavily research-verified effects of cruciferous vegetables on a bunch of liver-centered detoxification pathways, so much so that eating broccoli daily can lead to a literal multifold increase in urinary excretion of toxic metabolites! In other words, eating broccoli is known to make your body get rid of toxic material.
And the DIM derived from broccoli is just one small part of the multifaceted effect that broccoli has on your body’s toxic load.
The problem is in isolating DIM from the rest of estrogen metabolism.
When you do that, you are essentially using DIM pharmacologically, i.e. it’s not really that different from taking any other medication that targets just one (or even several) very specific biological pathway(s) in a reasonably predictable manner.
This is not always dangerous, but it can indeed be problematic for those people with DOWNSTREAM problems with estrogen metabolism.
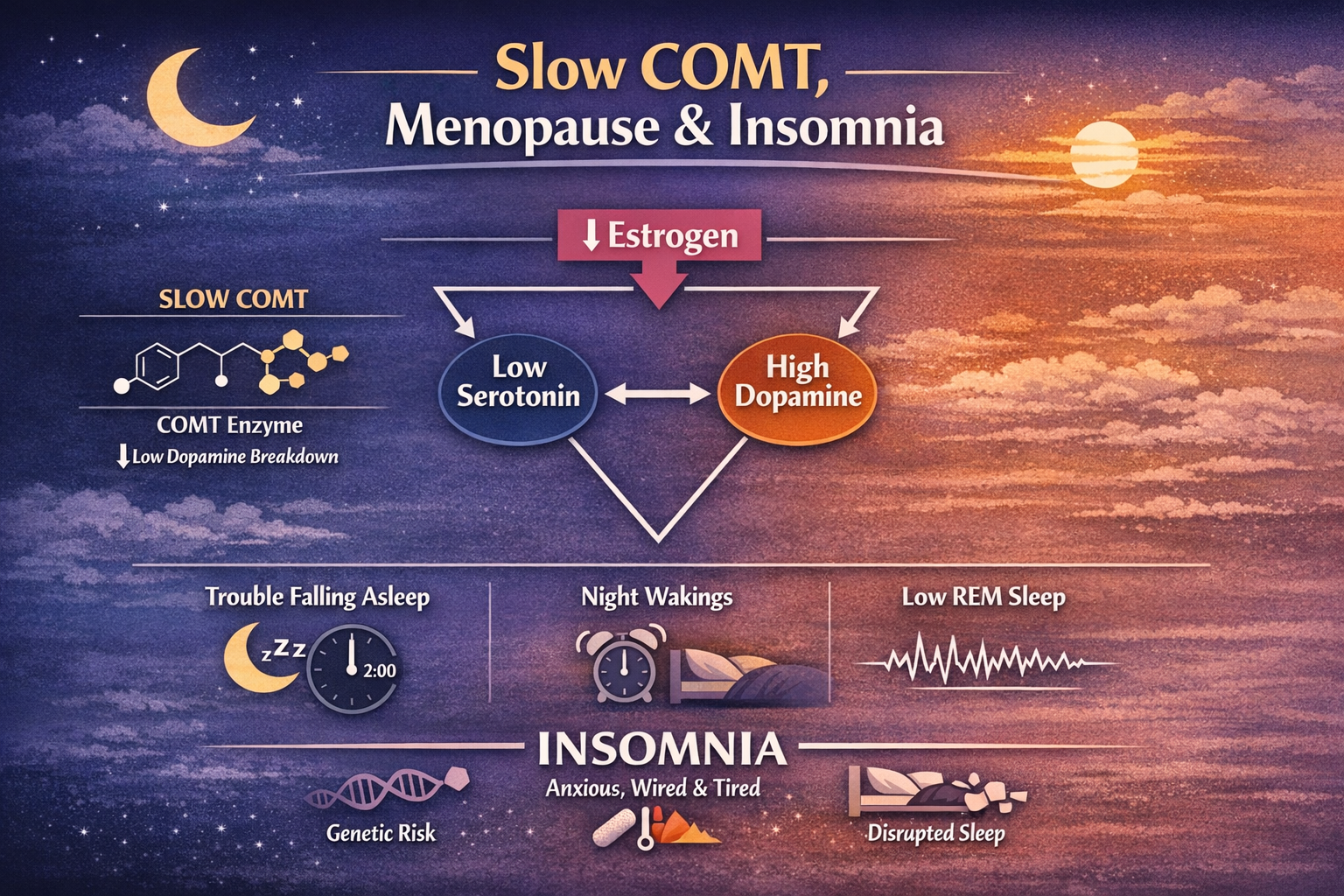
This very importantly includes those with Slow COMT deficits, which I have personally estimated symptomatically affect around 1 in 16 people, or 500 million people total.
Therefore if you have Slow COMT, please be extra wary of DIM supplementation (of course, this is not a recommendation), and ensure that you address downstream estrogen metabolism before using DIM.
In the liver, estrogen undergoes two phases of metabolism:
i.e. it’s broken down in two consecutive stages, first Phase 1, then Phase 2. You cannot switch it around and do Phase 2 before Phase 1 (it’s just not possible), and even more crucially, these two phases run in step with each other.
In other words, Phase 1 and Phase 2 must be occurring at roughly the same rate to ensure that everything pumped out of Phase 1 is then likewise eaten up and pumped out by Phase 2, to put it crudely.
Generally speaking, your body does this automatically.
BUT for those people with symptoms or consequential variants of genes that affect one of these phases, this can’t be taken for granted.
This is more of a problem if the genetic (or functional) problem is in Phase 2 metabolism, specifically because it you slow down the downstream components of estrogen metabolism, everything upstream gets (again, crudely) backed up, and those backed up intermediates are reactive and potentially harmful to your body.
The first phase of metabolism involves liver detox enzymes in the CYP family. And medical student will have heard of them because of their involvement in metabolizing a bunch of pharmaceuticals too.
In that first phase, these CYP enzymes break down estrogen into hydroxy-estrogen intermediates that then subsequently have to be broken down by Phase 2.
Phase 2 of estrogen metabolism is very largely run by COMT (among other enzymes).
So, for example, if you’re taking DIM but you have genetically Slow COMT (that you haven’t addressed sufficiently addressed!), then that means you’re speeding up Phase 1 estrogen breakdown while Phase 2 is “clogged,” and you’re likely building up those potentially harmful, reactive estrogen intermediates that sit in the middle!
And, even further, you won’t be properly channeling estrogen metabolism, so the estrogen overload you’re dealing with—whether endogenous or due to improperly timed HRT—will not actually be addressed by your DIM supplementation!
That all goes to say that you simply must address downstream estrogen metabolism prior to anything that affects upstream metabolism.
Don’t take DIM until you’ve fixed slow COMT, if you have it.
And (sorry to advertise) you can test for slow COMT with either of my home delivery Methylation Panel or Mood Panel genetic tests.
And if you’re still estrogen-symptomatic, there’s a reasonably good chance that you do have Slow COMT. You can do my Slow COMT Roadmap to take care of that, and I also have an Estrogen Overload-specific roadmap included within that subscription.
A Subtlety of Nature…

If you’ll allow me, I’d like to also point out a little subtlety here:
In my opinion, DIM is less of a potential problem when consumed as part of a cruciferous vegetable than it is when consumed as a supplement.
In cruciferous vegetables, it’s actually in the form of I3C (which you can also get as a supplement), which then later breaks down into DIM. And most importantly, you’ll be consuming it alongside hundreds of other factors that do in fact modulate Phase 2 liver metabolism, sulforaphane most obviously among them.
So the natural “package” that is broccoli more properly balances these various detoxification factors such that you’re not brutely speeding up certain elements of metabolism while neglecting other elements.
That’s not at all to say that DIM supplementation is not useful! Or that consuming broccoli solves all estrogen overload problems. Quite the contrary. But knowing absolutely nothing else, broccoli would be better than DIM done alone.
Check out my other articles (including many Slow COMT-specific ones):









Absolutely nothing in this article or on this website should be construed as medical advice! I am not your doctor. Thoroughly discuss all information and all potential changes with your doctor.
5th question I received:
“I would like to find out more about the fatigue caused by the slow COMT gene and how to fix it thank you.”